Common Tests During Pregnancy
These are some of the more common tests done during pregnancy.
First trimester prenatal screening tests
First trimester screening is a combination of fetal ultrasound and maternal blood testing. It can help find out the risk that the fetus has certain birth defects. Screening tests may be used alone or with other tests.
First trimester screening has 3 parts.
Ultrasound test for fetal nuchal translucency (NT)
Nuchal translucency screening uses an ultrasound test to check the area at the back of the fetal neck for extra fluid or thickening.
Two maternal serum (blood) tests
These tests measure 2 substances found in the blood of all pregnant women:
-
Pregnancy-associated plasma protein screening (PAPP-A). This is a protein made by the placenta in early pregnancy. Abnormal levels are linked to a higher risk for chromosome problems.
-
Human chorionic gonadotropin (hCG). This is a hormone made by the placenta in early pregnancy. Abnormal levels are linked to a higher risk for chromosome problems.
When used together, these tests have a greater ability to find out if the fetus might have a genetic birth defect, such as Down syndrome (trisomy 21) and trisomy 18.
If the results of these tests are abnormal, your healthcare provider will suggest genetic counseling. You may need more testing. That may include chorionic villus sampling, amniocentesis, cell-free fetal DNA, or other ultrasounds.
Second trimester prenatal screening tests
Second trimester prenatal screening may include several blood tests. These are called multiple markers. They give information about a woman's risk of having a baby with certain genetic conditions or birth defects. Screening is often done by taking a sample of your blood between the 15th and 20th weeks of pregnancy. The 16th to 18th is ideal. The multiple markers are listed below.
Alpha-fetoprotein screening (AFP)
This blood test measures the level of alpha-fetoprotein in your blood during pregnancy. AFP is a protein normally made by the fetal liver. It is in the fluid around the fetus (amniotic fluid) and crosses the placenta into your blood. The AFP blood test is also called MSAFP (maternal serum AFP). Abnormal levels of AFP may be a sign of:
-
Open neural tube defects (ONTD), such as spina bifida
-
Down syndrome
-
Other chromosome problems
-
Problems in the abdominal wall of the fetus
-
Twins
-
An incorrect due date
Other markers
Other markers are:
-
hCG. This is human chorionic gonadotropin hormone. It's made by the placenta.
-
Estriol. This is a hormone made by the placenta.
-
Inhibin. This is a hormone made by the placenta.
Abnormal results of AFP and other markers may mean you need more testing. An ultrasound is often done to confirm the dates of the pregnancy. It also looks at the fetal spine and other body parts for problems. You may need an amniocentesis for accurate diagnosis.
Multiple marker screening is not diagnostic. This means it is not 100% accurate. It's only a screening test to find out who should be offered more testing for their pregnancy. The tests show false-positive results. This means they show a problem when the fetus is actually healthy. Or the results may be false negative. This means they show that the fetus is normal when the fetus actually does have a health problem.
Having both first and second trimester screening tests done makes it more likely to find a problem, if there is one, than using just one screening alone. As many as 19 out of 20 cases of Down syndrome can be found when both first and second trimester screening are used.
What is an amniocentesis?
An amniocentesis is a test that takes a small sample of the amniotic fluid. It's done to diagnose chromosome problems and open neural tube defects (ONTDs), such as spina bifida. The test can also look for other genetic problems and disorders if you have a family history of them. These other results also depend on the lab doing the testing. An amniocentesis is generally offered to women between the 15th and 20th weeks of pregnancy who are at higher risk for chromosome problems. This includes women who have had an abnormal maternal blood screening test. The test may have indicated a higher risk for a chromosome problem or neural tube defect.
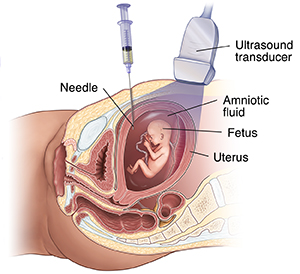
How is an amniocentesis done?
An amniocentesis involves putting a long, thin needle through your abdomen into the amniotic sac. The healthcare provider withdraws a small sample of the amniotic fluid. The amniotic fluid has cells shed by the fetus. These cells have genetic information. The specific details of each test vary slightly, but an amniocentesis often follows this process:
-
The healthcare team cleans your belly (abdomen) with an antiseptic.
-
The healthcare provider may use a local anesthetic to numb the skin.
-
The provider uses ultrasound to help guide a hollow needle into the amniotic sac.
-
The provider withdraws a small sample of fluid to be sent to a lab.
After the test, don't do any strenuous activity for 24 hours. You may feel some cramping during or after the amniocentesis.
If you are carrying twins or other multiples, you will need sampling from each amniotic sac to study each baby.
The fluid sample is sent to a genetics lab so that the cells can grow and be tested. AFP is also measured to rule out an open neural tube defect, such as spina bifida. AFP is a protein made by the fetus and is in the fluid.
Results are often available in 10 days to 2 weeks, depending on the lab.
Discuss the risks of this procedure with your healthcare provider. Sometimes the amniocentesis can't be done. It depends on the position of the baby, the placenta, the amount of fluid, and your anatomy.
What is a chorionic villus sampling (CVS)?
Chorionic villus sampling (CVS) is a prenatal test. It involves taking a sample of some of the placental tissue. This tissue often has the same genetic material as the fetus. It can be tested for chromosome problems and some other genetic problems. The test can also look for other genetic problems and disorders if you have a family history of them. These other results also depend on the lab doing the testing. Unlike amniocentesis, CVS does not give information on neural tube defects, such as spina bifida. For this reason, women who have CVS also need a follow-up blood test between 16 and 18 weeks of their pregnancy to screen for neural tube defects.
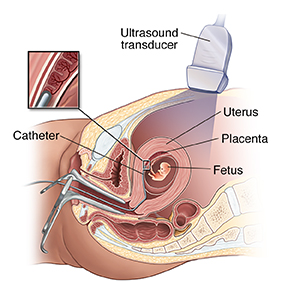
How is CVS done?
CVS may be offered if you are at higher risk for chromosome problems. You may also be offered it if you have a family history of a genetic problem diagnosed by testing the placental tissue. CVS is usually done between the 10th and 13th weeks of pregnancy. The exact method for CVS can vary, but the procedure involves putting a small tube (catheter) through your vagina and into your cervix. It usually follows this process:
-
The healthcare provider uses ultrasound to guide the catheter into place near the placenta.
-
The provider removes tissue using a syringe on the other end of the catheter.
-
For a transabdominal CVS, the provider puts a needle through your abdomen and into the uterus to take a sample of cells from the placenta.
-
You may feel some cramping during and after the CVS procedure.
If you are carrying twins or other multiples, you often will need sampling from each placenta. But CVS is not always advised for multiples because the procedure is complicated, and the placentas may not be in a good position to get a sample.
The tissue samples are sent to a genetic lab to grow and be tested. Results are often available in 10 days to 2 weeks, depending on the lab.
Some women may not be candidates for CVS, or they may not get results that are 100% accurate. They may need a follow-up amniocentesis. In some cases, an active vaginal infection, such as herpes or gonorrhea, will prohibit the procedure. Other times, the healthcare provider takes a sample that does not have enough tissue to grow in the lab. That may cause incomplete or inconclusive results.
Discuss the risks of CVS with your healthcare provider.
What is fetal monitoring?
During late pregnancy and during labor, your healthcare provider may want to watch the fetal heart rate and other functions. Fetal heart rate monitoring is a way of checking the rate and rhythm of the fetal heartbeat. The average fetal heart rate is between 110 and 160 beats per minute. It may change as the fetus responds to conditions in the uterus. An abnormal fetal heart rate or pattern may mean that the fetus is not getting enough oxygen or there are other problems. It also may mean that an emergency or cesarean delivery is needed.
How is fetal monitoring done?
The most basic type of fetal heart rate monitor is to use a type of stethoscope called a fetoscope. Another type of monitoring is with a hand-held Doppler device. This is often used during prenatal visits to count the fetal heart rate. During labor, continuous electronic fetal monitoring is often used. The specific details may vary slightly, but electronic fetal monitoring often follows this process:
-
The healthcare provider puts gel on your abdomen to help the ultrasound transducer work correctly.
-
The provider attaches the ultrasound transducer to the abdomen with straps and sends the fetal heartbeat to a recorder. The fetal heart rate is displayed on a screen and may be printed onto special paper.
-
During contractions, a monitoring device (external tocodynamometer) is placed over the top of the uterus with a belt. This device can record the patterns of contractions.
Sometimes, internal fetal monitoring is needed for a more accurate reading of the fetal heart rate. This monitoring can be done when birth is close. Your amniotic sac must be broken, and your cervix must be partially dilated to do it. Internal fetal monitoring involves putting an electrode through the dilated cervix. The electrode is attached to the scalp of the fetus.
What are glucose tolerance tests and the glucose challenge?
The first 1-hour test is a glucose challenge test. If the results are abnormal, a glucose tolerance test is done.
A glucose tolerance test is often done in weeks 24 to 28 of pregnancy. It measures levels of sugar (glucose) in your blood. Abnormal glucose levels may be a sign of gestational diabetes.
How is a glucose tolerance test done?
The glucose tolerance test is done if you have an elevated 1-hour glucose challenge test.
The specific details may vary slightly, but a glucose tolerance test often follows this process:
-
You may be asked to drink only water on the day you get the test.
-
The healthcare provider will draw a fasting sample of blood from a vein.
-
You will be given a special glucose solution to drink.
-
The provider will draw blood several times over several hours to measure the glucose levels in your body.
What is a group B strep culture?
Group B streptococcus (GBS) are bacteria found in the lower genital tract of about 1 in 4 women. GBS infection often causes no problems in women before pregnancy. But it can cause serious illness in the mother during pregnancy. GBS may cause chorioamnionitis. This is a severe infection of the placental tissues. It can also cause postpartum infection. Urinary tract infections caused by GBS can lead to preterm labor and birth, or pyelonephritis and sepsis.
GBS is the most common cause of life-threatening infections in newborns, including pneumonia and meningitis. Newborn babies get the infection during pregnancy or from the mother's genital tract during labor and birth.
The CDC advises that all pregnant women be screened for vaginal and rectal group B strep between 35 to 37 weeks gestation. If you have certain risk factors or a positive result, you should be treated with antibiotics. This will lower the risk of passing GBS to your baby. Babies whose mothers get antibiotics for a positive GBS test are 20 times less likely to develop the disease than those whose mothers don't get treatment.
What is an ultrasound?
An ultrasound scan is a test that uses high-frequency sound waves to make pictures of the internal organs. A screening ultrasound is sometimes done during a pregnancy to check normal fetal growth and make sure of the due date. Ultrasounds may be done at various times throughout pregnancy for many reasons.
In the first trimester
-
To find out the due date. This is the most accurate way of finding the due date.
-
To find out the number of fetuses and see the placenta(s)
-
To diagnose an ectopic pregnancy or miscarriage
-
To look at the uterus and other pelvic anatomy
-
In some cases, to find fetal problems
Midtrimester (sometimes called the 18- to 20-week scan)
-
To confirm the due date. A due date set in the first trimester is rarely changed.
-
To find out the number of fetuses and look at the placentas
-
To help with prenatal tests, such as an amniocentesis
-
To look at the fetal anatomy to see if there are any problems
-
To check the amount of amniotic fluid
-
To look at blood flow patterns
-
To watch fetal behavior and activity
-
To look at the placenta
-
To measure the length of the cervix
-
To check fetal growth
Third trimester
-
To check fetal growth
-
To check the amount of amniotic fluid
-
To complete a biophysical profile
-
To find out the position of a fetus
-
To check the placenta
How is an ultrasound scan done?
The specific details may vary slightly, but ultrasounds often follow the same process. Two types of ultrasounds can be done during pregnancy:
-
Abdominal ultrasound. In an abdominal ultrasound, the healthcare provider puts gel on your abdomen. The ultrasound transducer glides over the gel to create the image.
-
Transvaginal ultrasound. In a transvaginal ultrasound, the provider uses a smaller ultrasound transducer. They put the transducer into the vagina and rest it against the back of the vagina to create an image. A transvaginal ultrasound makes a sharper image. It is often used in early pregnancy.
There are several types of ultrasound imaging methods. The most common is 2-D. This gives a flat picture of one aspect of the image.
If more information is needed, a 3-D ultrasound exam can be done. This method gives a 3-D picture. It needs a special machine and special training. But the 3-D image lets the healthcare provider see width, height, and depth of images. These can be helpful in diagnosis. The 3-D images can also be saved for later review.
The latest technology is 4-D ultrasound. It lets the healthcare provider see the fetus moving in real time. With 4-D imaging, a 3-D image is continuously updated. This makes a "live action" view. These images often have a golden color that helps show shadows and highlights.
Ultrasound images may be captured in still photographs or on video to document findings.
Ultrasounds are constantly being improved and refined. As with any test, results may not be completely accurate. But ultrasound can give valuable information for parents and healthcare providers to help manage and care for the pregnancy and fetus. Ultrasound also gives parents a special chance to see their baby before birth. This helps them to bond and establish an early relationship.
What are the risks and benefits of ultrasound?
Fetal ultrasound has no known risks other than mild discomfort. This is because of pressure from the transducer on the abdomen or in the vagina. No radiation is used during the procedure.
Transvaginal ultrasound needs the ultrasound transducer to be covered in a plastic or latex sheath. This may cause a reaction in women with a latex allergy.
Fetal ultrasound is sometimes offered in nonmedical settings to give keepsake images or videos for parents. The ultrasound procedure itself is considered safe, but it's possible that untrained workers may give parents false assurances about their baby's well-being. Or perhaps a problem may be missed. Having ultrasound done by trained medical staff who can correctly understand findings is recommended. Talk with your healthcare provider or midwife if you have questions.
What is genetic carrier screening?
Many genetic problems can be diagnosed before birth. Your healthcare provider or midwife may advise genetic testing during the pregnancy if you or your partner have a family history of genetic disorders, or you have had a fetus or baby with a genetic problem.
Examples of genetic disorders that are commonly screened for include: